Print(PDF/596KB) Jun. 09, 2023 R&D
Generation and purification of ACTH-secreting hPSC-derived pituitary cells for effective transplantation
Key Points
- Successful differentiation from hESCs and hiPSCs to robust and highly efficient pituitary-hypothalamic tissues as development for human clinical use.
- Successful generation of high-purity pituitary hormone-producing cells by cell sorting using EpCAM.
- Transplantation into hypopituitary mice confirmed long-term efficacy and secretion control in response to the environment.
- Expected to contribute to regenerative medicine for patients with hypopituitarism.
Summary
A joint research team led by joint researcher Shiori Taga (Sumitomo Pharma Co., Ltd., 1st author), Associate Professor Hidetaka Suga (corresponding author), and Professor Hiroshi Arima in Department of Diabetes and Endocrinology, Nagoya University Graduate School of Medicine, and Group Manager Atsushi Kuwahara in Regenerative & Cellular Medicine Kobe Center, Sumitomo Pharma Co., Ltd., and Chief Researcher Tokushige Nakano in Environmental Health Science Laboratory, Sumitomo Chemical Co., Ltd., and Professor Hiroshi Nagasaki, in School of Medicine, Fujita Health University established a highly efficient and robust method for generating pituitary hormone-producing cells using human embryonic stem cells (hESCs) and human induced pluripotent stem cells (hiPSCs).
The pituitary gland plays a critical role in controlling various hormones, among which physiological adrenocorticotropic hormone (ACTH) requirements fluctuate with circadian rhythms and various stress. Current replacement therapy for hypopituitarism cannot match supply to this fluctuating demand, which may affect life prognosis.
This joint research group previously succeeded in inducing the pituitary-hypothalamus tissues from hESCs in 2016 and from hiPSCs in 2020. In this study, we improved these methods to stably and efficiently generate pituitary-hypothalamus tissue from human ES cells and human iPS cells. Furthermore, adding cell sorting using EpCAM, a pituitary surface antigen marker, made it possible to generate high-purity pituitary hormone-producing cells (3D-pituitaries). When transplanted into hypopituitary mice, engrafted 3D-pituitaries survived for half a year during which blood ACTH levels were improved. Furthermore, hormone secretion control and response to pseudo-infection stress were confirmed.
This method of generating purified pituitary tissue opens new avenues of research for pituitary regenerative medicine.
Research Background
The pituitary gland plays a critical role in controlling various hormones and a wide variety of life phenomena such as homeostasis, growth, metabolism, stress response, and reproduction. Therefore, when the function of pituitary hormone-producing cells declines, various symptoms appear. The lack of ACTH can cause adrenal insufficiency and can be life-threatening. Hormone replacement is the current therapy against hypopituitarism. However, there remains a problem that the current replacement therapy cannot sufficiently cope with the fluctuating hormone requirements. It is difficult to avoid both the risk of adrenal insufficiency due to hormone deficiency and the risk of diabetes and hypertension by excessive hormones. If we can create hormone-producing cells that can respond to the surrounding environment and refine them suitably for clinical use, it may become a better treatment than the replacement therapy.
This research group succeeded in inducing the pituitary-hypothalamus tissues from hESCs in 2016 and from hiPSCs in 2020. In order to realize regenerative medicine, it was necessary to efficiently produce highly pure pituitary hormone-producing cells, assuming standards that could be used in human clinical practice. In this report, we attempted to generate highly efficient and pure pituitary hormone-producing cells from hESCs and hiPSCs.
Research Results
The differentiation methods for pituitary-hypothalamic tissues reported in 2016 and 2020 are characterized by reproducing the formation of these sites in the embryo in vitro. In developing a method for inducing pituitary-hypothalamic tissues for human clinical use, we aimed to more precisely reproduce pituitary development in vitro, and created pituitary-hypothalamic tissues by additionally treating hESCs and hiPSCs with inhibitors of Wnt and TGFβ signaling pathways (Fig. 1). As a result, almost all aggregates in the generated pituitary-hypothalamic tissues contained ACTH-producing cells, which improved stability and efficiency compared to approximately 30% in the previous culture method.
Fig.1
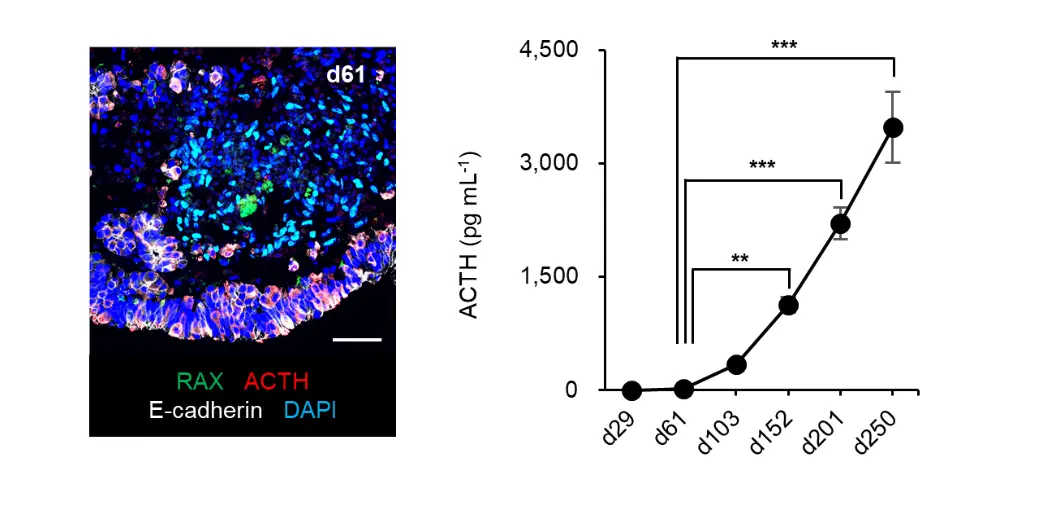
Fig.1 Pituitary-hypothalamus tissues generated from hESCs
The left figure shows mature pituitary-hypothalamic tissues, with the pituitary gland (white) containing ACTH-producing cells (red) in the outer layer of the aggregates, and the hypothalamus (green) in the inner layer. The right graph shows ACTH secretory capacity of the pituitary-hypothalamic tissues.
However, even with this differentiation method, there remains the problem that it is difficult to strictly and consistently control the induction to the pituitary gland and hypothalamus in the pituitary-hypothalamus tissues, especially the latter. Therefore, we aimed to generate highly pure pituitary tissues by performing cell sorting using EpCAM, a pituitary surface antigen marker, and isolating only pituitary hormone-producing cells from the pituitary-hypothalamic tissues. After examining various conditions, we found that cell sorting after day 60 is desirable.
The reaggregated cells after purification (3D-pituitaries) consisted highly pure pituitary hormone-producing cells rich in ACTH-producing cells, and showed high ACTH secretory capacity in vitro. We examined whether this 3D-pituitaries is subject to the same regulation as in vivo and secretes pituitary hormones in vitro. We confirmed that ACTH secretion increased after adrenocorticotropin-releasing hormone (CRH) stimulation, while suppressed upon dexamethasone treatment (Fig. 2).
Fig.2
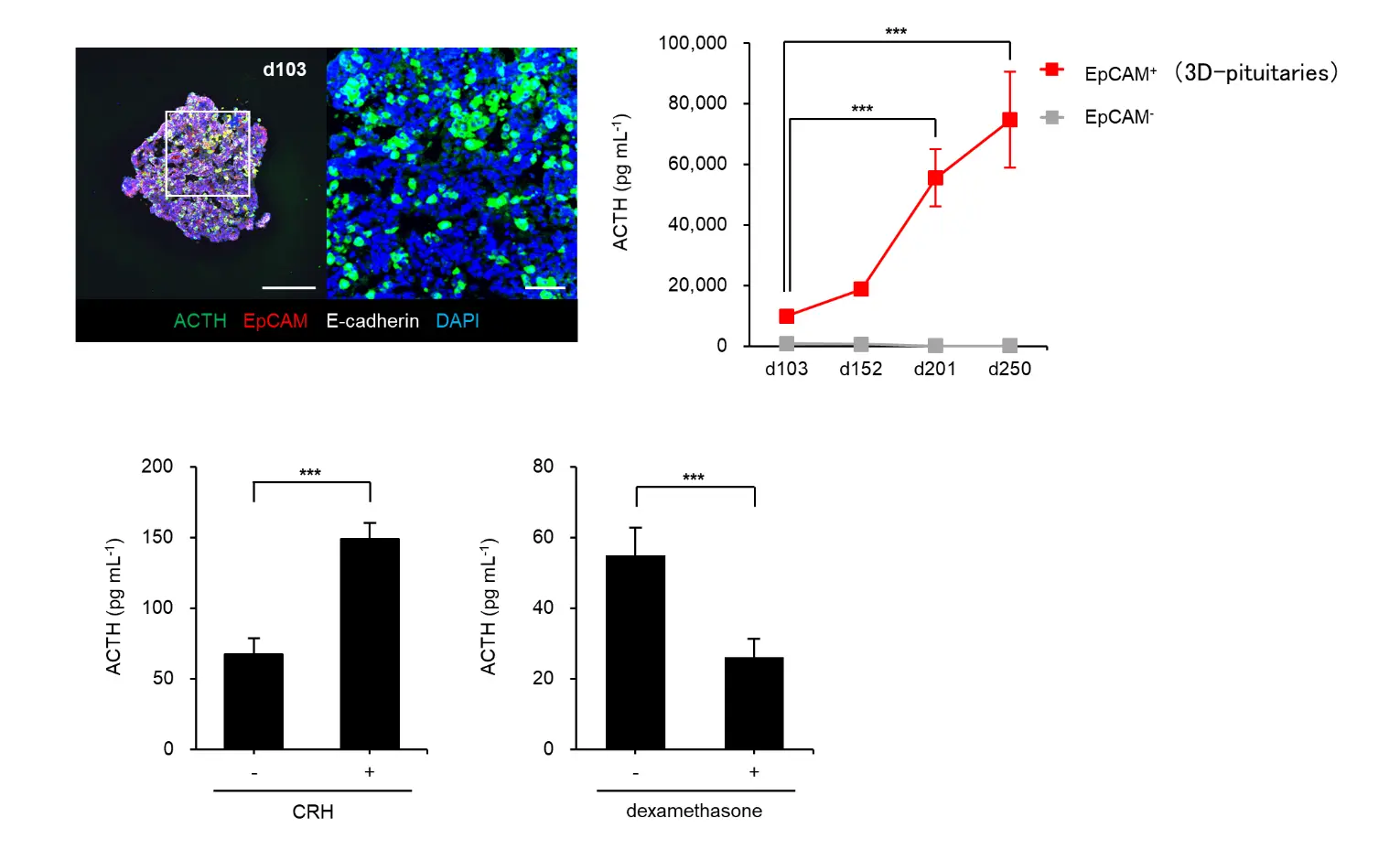
Figure 2: 3D-pituitaries and evaluation of hormone-secreting function in vitro
The upper figures (left) show reaggregated pituitary hormone-producing cells after purification. The entire aggregate is composed of pituitary cells (red and white) and contains many ACTH-producing cells (green).
The upper graph (right) shows that ACTH secretory capacity of 3D-pituitaries improved in long-term culture in vitro. The lower graph shows that ACTH secretion is increased in response to CRH (left), and is suppressed in response to dexamethasone (right).
Next, in order to confirm whether this 3D-pituitaries functions in vivo after transplantation, we transplanted 3D-pituitaries into hypopituitary mice.
The transplanted cells survived in mice for more than half a year, and improved blood ACTH levels. Further examination of hormonal responsiveness suggested that it also possessed responsiveness to the environment. For example, in the dexamethasone-treated transplanted mice, transplanted cells were properly suppressed, and ACTH was not secreted. This result suggests that 3D-pituitaries receive steroid feedback through the systemic circulation and secretion stops when it should stop even after transplantation. Risk of side effects caused by excessive secretion from transplanted cells is low. Those responses’ maintenance in vivo after transplantation, a feature of great clinical importance, is first documented here. In addition, we measured blood ACTH response to the mock-infection stress of lipopolysaccharide (LPS) administration. ACTH secretion increased in response to LPS in the transplanted mice. It suggests that it is possible to reduce acute adrenal-insufficiency risk by increasing the secretion of ACTH from the graft during “sick days”, rapidly life-threatening conditions for ACTH-deficient patients in human clinical practice (Fig. 3).
Fig.3
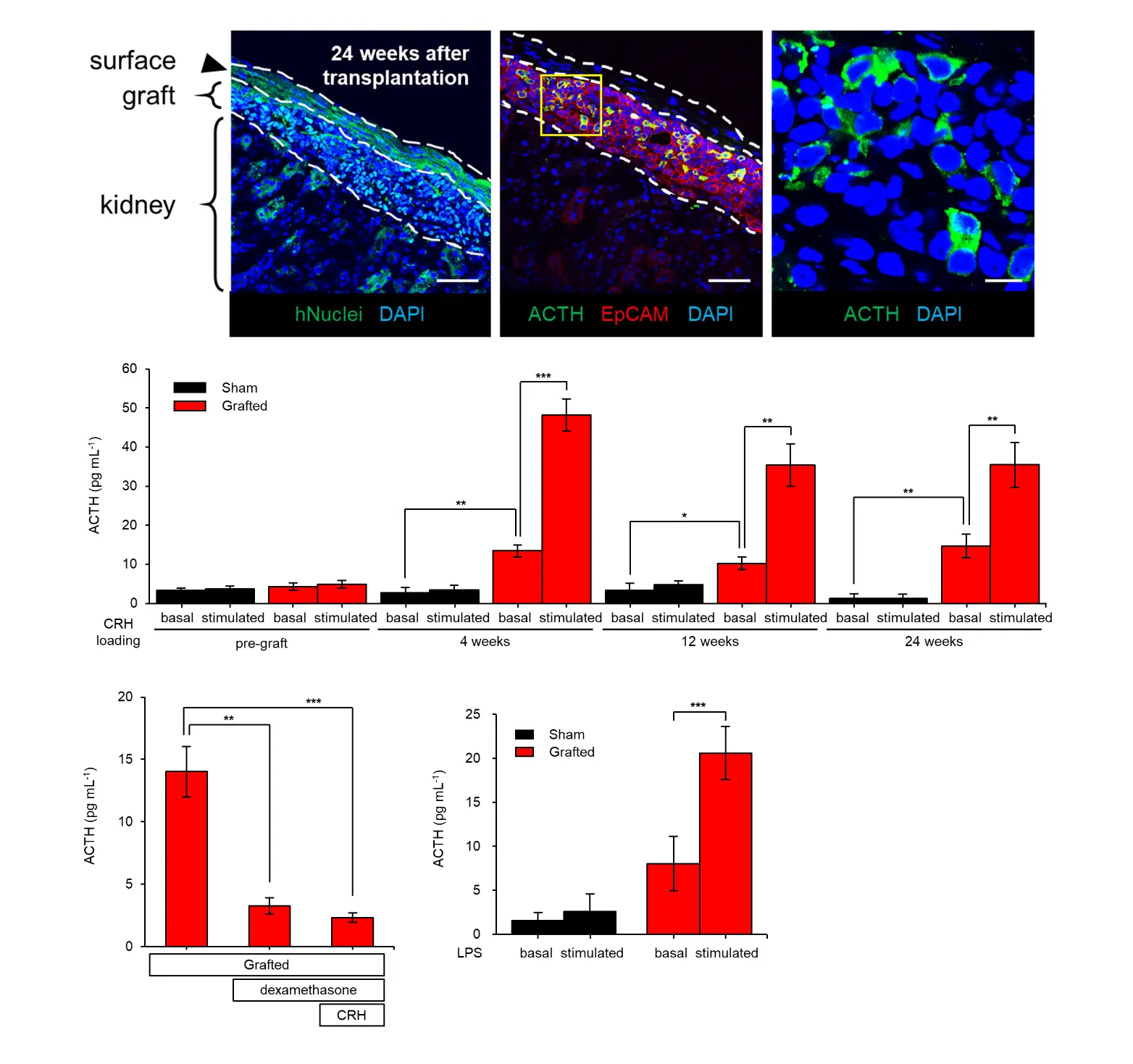
Figure 3: Efficacy of 3D-pituitaries transplantation into hypopituitary mice
The upper three figures show the transplanted cells 24 weeks after transplantation. Human nuclei-positive cells (green, left), pituitary cells (red, middle), and ACTH-producing cells (green, middle and right) are shown. It shows that hPSC-derived 3D-pituitariess are properly engrafted in the transplantation site. The middle figure shows the blood ACTH concentration in the transplanted group compared to the sham-operated group. The blood ACTH concentration improved by transplantation (basal), and that ACTH increased after CRH stimulation (stimulated). This effect was observed up to 24 weeks after transplantation. The lower graph (left) shows that ACTH secretion is suppressed by dexamethasone treatment (middle bar graph). ACTH secretion remained suppressed even when CRH stimulation was added to the suppression by dexamethasone treatment (right bar graph). The lower graph (right) shows that LPS administration increases ACTH secretion.
Research Summary and Future Perspective
By making it possible to generate highly efficient and highly pure pituitary hormone-producing cells from hESCs and hiPSCs, we have taken a step forward toward the practical application of regenerative medicine for patients with impaired pituitary function. In the future, based on the results of this research, we will examine clinical protocols such as clinical administration methods and concomitant drugs, manufacturing methods such as large-scale production of clinical cells with higher efficiency, and non-clinical safety evaluations. We will proceed with research and development toward the realization of regenerative medicine for the pituitary gland.
Publication
Shiori Taga1,2, Hidetaka Suga1, Tokushige Nakano3, Atsushi Kuwahara2, Naoko Inoshita4, Yu Kodani5, Hiroshi Nagasaki5, Yoshitaka Sato6, Yusuke Tsumura7, Mayu Sakakibara1, Mika Soen1, Tsutomu Miwata1, Hajime Ozaki1, Mayuko Kano8, Kenji Watari2, Atsushi Ikeda2, Mitsugu Yamanaka9, Yasuhiko Takahashi3, Sachiko Kitamoto3, Yohei Kawaguchi1, Takashi Miyata1, Tomoko Kobayashi1, Mariko Sugiyama1, Takeshi Onoue1, Yoshinori Yasuda1, Daisuke Hagiwara1, Shintaro Iwama1, Yoshitaka Tomigahara3*, Toru Kimura2, and Hiroshi Arima1
- 1Department of Endocrinology and Diabetes, Graduate School of Medicine, Nagoya University, Nagoya, Aichi 466-8550, Japan.
- 2Regenerative & Cellular Medicine Kobe Center, Sumitomo Pharma Co., Ltd., Kobe, Hyogo 650-0047, Japan.
- 3Environmental Health Science Laboratory, Sumitomo Chemical Co., Ltd., Osaka 554-8558, Japan.
- 4Department of Pathology, Moriyama Memorial Hospital, 4-3-1 Kitakasai, Edogawa-ku, Tokyo 134-0081, Japan.
- 5Department of Physiology, School of Medicine, Fujita Health University, Toyoake, Aichi 470-1192, Japan.
- 6Department of Virology, Graduate School of Medicine, Nagoya University, Nagoya, Aichi 466-8550, Japan.
- 7Department of Pediatrics, Graduate School of Medicine, Nagoya University, Nagoya, Aichi 466-8550, Japan.
- 8Division of Metabolism and Endocrinology, Department of Internal Medicine, St. Marianna University School of Medicine, Kawasaki, Kanagawa 216-8511, Japan
- 9Drug Research Division, Sumitomo Pharma Co., Ltd., Osaka 554-0022, Japan.
- *Present affiliation: Nihon Medi-Physics Co., Ltd.
DOI:10.1016/j.stemcr.2023.05.002
Inquiries from the Press